Autoimmune disorders that affect the brain can take many forms beyond the most well-known example of multiple sclerosis (MS). Autoimmune encephalitis and autoimmune epilepsy can also occur, but like MS, their etiology is unknown. It has been suggested that autoimmune diseases like lupus and rheumatoid arthritis, among others, may be triggered by viral infections in addition to other environmental factors and genetic factors (Toussirot and Roudier, 2008). In light of these considerations, we must be vigilant for autoimmune disorders linked to SARS-CoV-2 infection.
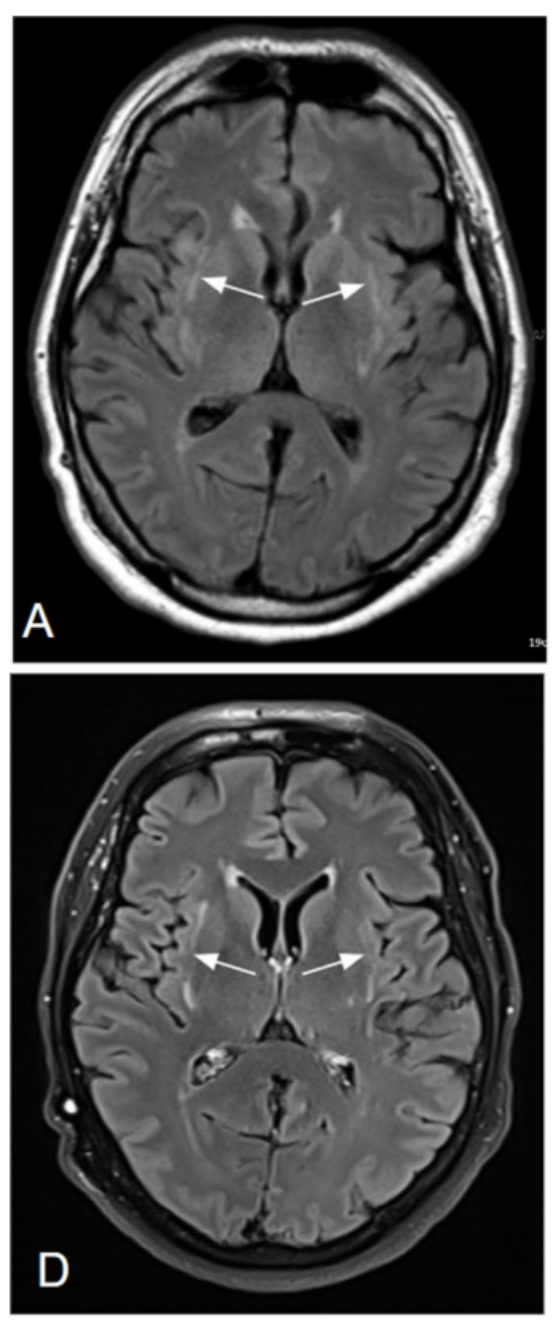
A case report published recently in the Journal of Neurology describes autoimmune encephalitis in a case of severe COVID-19 (Zuhorn et al., 2020). A 54-year-old Caucasian man presented to clinic with cough, fever, and weakness and was diagnosed with COVID-19 by a positive RT-PCR on nasopharyngeal swab sample. On day 3 after symptom onset, the patient was admitted to the hospital with symptoms of aggression, disorientation, stupor, and respiratory deterioration, which were thought to be part of COVID-19 encephalitic syndrome. Blood gas and lung sound analysis ruled out hypoxemia. The patient’s medical history included obesity, arterial hypertension and obstructive sleep apnea. Chest CT revealed bilateral lung infiltrates. The patient was intubated on day 4 due to respiratory deterioration. After eight days, the patient was extubated and at this point tested negative for SARS-CoV-2; however, the patient was still delirious and had difficulty concentrating. MRI revealed altered signals in claustrum with reduced diffusion. CSF analysis revealed lymphocytic pleocytosis and was “negative for common neurotropic viruses” as well as SARS-CoV-2. Serum and CSF also tested negative for antineuronal antibodies and the CSF was negative for antibodies against SARS-CoV-2. By discharge date, the patient improved symptomatically though retained mild cognitive impairment.
Four months later, follow-up testing demonstrated normalization of cell counts in the CSF and improvement in imaging findings on brain MRI. Interestingly, the patient’s cognitive status returned to baseline though there were persistent claustrum lesions on brain MRI. The authors suggest that lack of direct CNS invasion of the SARS-CoV-2 virus and the presence of neuropsychiatric symptoms was evidence of parainfectious autoimmune encephalitis. Additionally, the unique pattern of the brain MRI in this patient, dubbed the claustrum sign, has been previously seen in MRIs of autoimmune epilepsy patients. Because the claustrum plays a key role in regulating consciousness, lesions within it correlate well with the symptoms seen in this case. As claustrum lesions have also been reported in autoimmune encephalitis, the authors believe that inflammation was key in mediating neurological damage in this case.
To my knowledge, this is one of the first case studies that explicitly suggests an autoimmune mechanism for COVID-19-related neurological symptoms. We have seen in other studies that COVID-19 has been correlated with stroke, seizures, and acute necrotizing encephalopathy, but none of those studies revealed whether the virus directly infiltrated the CNS and caused these symptoms. This case report suggests that the virus may be capable of initiating an autoimmune response that goes on to cause neurological damage.
References
Toussirot, É., & Roudier, J. (2008). Epstein–Barr virus in autoimmune diseases. Best practice & research Clinical rheumatology, 22(5), 883-896.
Zuhorn, F., Omaimen, H., Ruprecht, B., Stellbrink, C., Rauch, M., Rogalewski, A., … & Schäbitz, W. R. (2020). Parainfectious encephalitis in COVID-19:“The Claustrum Sign”. Journal of Neurology, 1-4.
Leave a Reply