April 5, 2020 by Sam Bazzi
Summary:
Currently, there is evidence to suggest that some patients suffering from COVID-19 experience a variety of neurological symptoms, including stroke, delirium, anosmia, epileptic seizures, vomiting, dizziness, and headache. It is unclear how or why these symptoms arise, but some clues exist based on previous coronavirus outbreaks (see Potential Mechanisms).
In Wuhan, China, a retrospective study done on 214 confirmed COVID-19 cases assessed neurological symptoms in patients. The cases were classified as severe (88, 41.1%) and non-severe (126, 58.9%). Severe patients were not only older and more likely to have underlying health problems but were also more likely to have neurological symptoms. 78 total patients had neurological symptoms, with 40 of them being severe cases (45.5%) and 38 of them being non-severe cases (30.2%) (Mao, et al., 2020).
According to Dr. Alessandro Pezzini, some COVID-19-positive patients in Italy are experiencing neurological symptoms including stroke, delirium, epileptic seizures, and others. A separate neuro-COVID-19 unit has been established to manage these patients (Talan, 2020).
Potential Mechanisms for Neurological Symptom onset:
- Previous SARS virus (SARS-CoV1) was reported to infect the brainstem in some patients as well as in experimental animals. Some coronaviruses are able to spread trans-synaptically through neurons from the mechanoreceptors and chemoreceptors in the lung to the medullary cardiorespiratory center. SARS-CoV-2 may operate in a similar manner(Li, et al., 2020).
- It is possible that the simple lack of oxygen and elevated level of CO2in the blood due to diminished respiratory function is primarily responsible for neurological symptoms.
- SARS-CoV-2’s main site of entry is angiotensin-converting enzyme 2 (ACE2). While predominantly present in the respiratory and gastrointestinal systems, ACE2 is also present in the CNS, specifically in neurons and glia (Gowrisankar, et al., 2020, Xia, Lazartigues, 2020). The brain regions where ACE2 is expressed are the brainstem and other regions that regulate cardiovascular function such as the subfornical organ, paraventricular nucleus, nucleus of the tractus solitarius, and rostral ventrolateral medulla. Some believe that SARS-CoV-2 may be able to enter the CNS via clathrin-mediated endocytosis into astrocytes, much in the same way that HEV 67N (another coronavirus) does, though there is no evidence yet for this claim (Steardo, et al., 2020). Contradicting this claim is a single case study so far that found no presence of the virus in the CSF of a COVID-19 patient (Filatov, et al., 2020).
- Some evidence exists that a cytokine storm is present in severe COVID-19 cases (Mehta, McAuley, and Brown, 2020). Intracranial cytokine storms can lead to blood-brain barrier breakdown (Poyiadji, et al., 2020), which could contribute to further virus infiltration and the development of neurological symptoms. How the cytokine storm initiates intracranially is unclear at this time.
Case Studies in the USA:
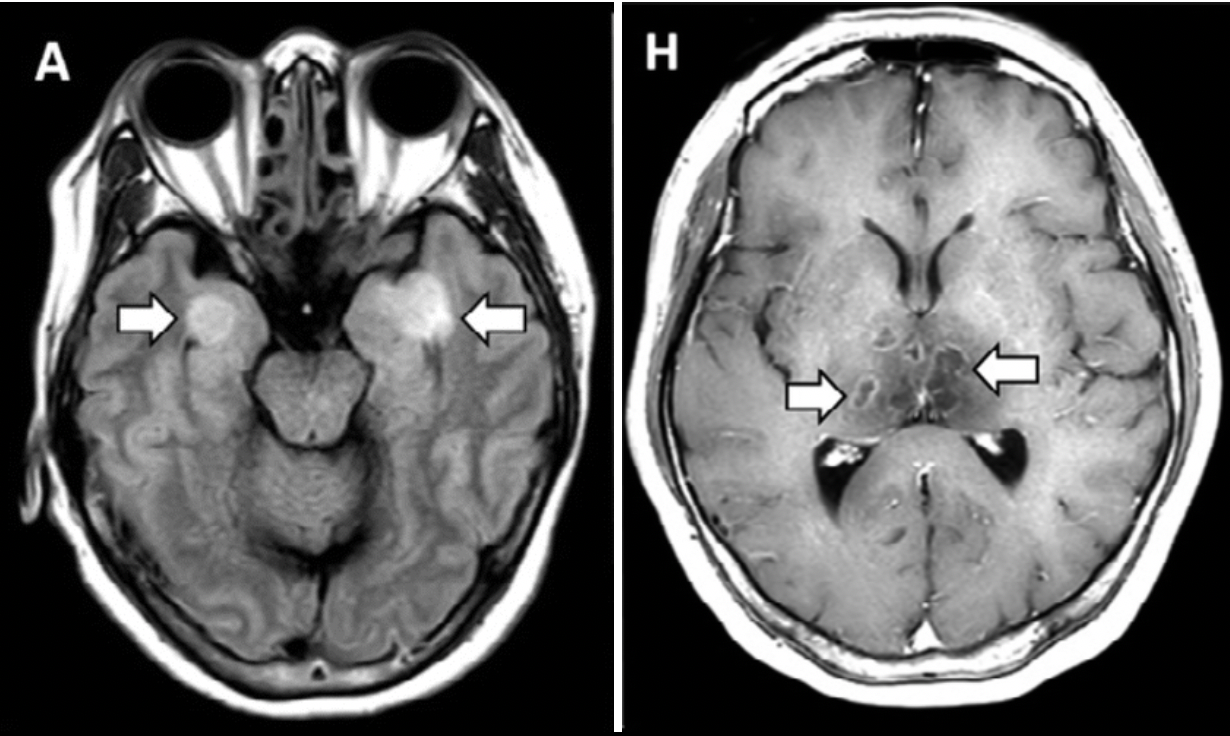
COVID-19–associated Acute Hemorrhagic Necrotizing Encephalopathy: CT and MRI Features. (Poyiadji, et al., 2020)
-
- Airline worker, female, in her 50s
- 3-day history of cough, fever, and altered mental status
- Tested negative for influenza, positive for COVID-19
- Tests for herpes simplex virus 1 and 2, varicella zoster virus, and West Nile virus were negative
- First presumptive case of COVID-19-associated acute necrotizing hemorrhagic encephalopathy, a rare encephalopathy that has been associated with other viral infections but has yet to be demonstrated as a result of COVID-19 infection
Neurological Complications of Coronavirus Disease (COVID-19): Encephalopathy. (Filatov, et al., 2020)
-
- 74-year old man from the Netherlands arrives in USA, presents symptoms within 1 week of arrival
- Past medical history of atrial fibrillation, cardioembolic stroke, Parkinson’s disease, chronic obstructive pulmonary disease (COPD), and recent cellulitis presented to the emergency department with a chief complaint of fever and cough. Tested positive for SARS-CoV-2.
- Due to the severe alteration in mental status, neurology service was consulted. Upon examination, the patient was found to be encephalopathic, nonverbal, and unable to follow any commands; however, he was able to moveall his extremities and was reacting to noxious stimuli.
- No virus found in CSF, so authors believe SARS-Cov 2 can not cross the blood-brain barrier or cause meningitis or encephalitis.
Additional Interesting Info
One study found that 29% of T-cells isolated from multiple sclerosis patients cross-reacted with both myelin basic protein and coronavirus antigens from a different human coronavirus (strain 229E), compared to only 1.3% of T-cells from control patients. This study established that some molecular mimicry exists between myelin proteins and pathogenic coronavirus proteins (Talbot, et al., 1996). This study lends some evidence to the idea that infectious insults could prime the immune system for subsequent autoimmunity.
Written by: Sam Bazzi
Edited by: Jina Zhou and Esther Melamed
4/5/2020
References
Filatov, A., Sharma, P., Hindi, F., & Espinosa, P. S. (2020) Neurological Complications of Coronavirus Disease (COVID-19): Encephalopathy. Cureus.
Gowrisankar, Y. V., & Clark, M. A. (2016). Angiotensin II regulation of angiotensin‐converting enzymes in spontaneously hypertensive rat primary astrocyte cultures. Journal of neurochemistry, 138(1), 74-85.
Li, Y. C., Bai, W. Z., & Hashikawa, T. (2020). The neuroinvasive potential of SARS‐CoV2 may be at least partially responsible for the respiratory failure of COVID‐19 patients. Journal of Medical Virology.
Mao, L., Wang, M., Chen, S., He, Q., Chang, J., Hong, C., … & Li, Y. (2020). Neurological Manifestations of Hospitalized Patients with COVID-19 in Wuhan, China: a retrospective case series study. The Lancet.
Mehta, P., McAuley, D. F., Brown, M., Sanchez, E., Tattersall, R. S., & Manson, J. J. (2020). COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet.
Poyiadji, N., Shahin, G., Noujaim, D., Stone, M., Patel, S., & Griffith, B. (2020). COVID-19–associated Acute Hemorrhagic Necrotizing Encephalopathy: CT and MRI Features. Radiology, 201187.
Steardo, L., Steardo, L., Zorec, R., & Verkhratsky, A. (2020). Neuroinfection may potentially contribute to pathophysiology and clinical manifestations of COVID‐19. Acta Physiologica.
Talan, J. (2020, March 27). COVID-19: Neurologists in Italy to Colleagues in US: Look for Poorly-Defined Neurologic Conditions in Patients with the Coronavirus. Neurology Today.
Talbot, P. J., Paquette, J. S., Ciurli, C., Antel, J. P., & Ouellet, F. (1996). Myelin basic protein and human coronavirus 229E cross‐reactive T cells in multiple sclerosis. Annals of neurology, 39(2), 233-240.
Xia, H., & Lazartigues, E. (2010). Angiotensin-converting enzyme 2: central regulator for cardiovascular function. Current hypertension reports, 12(3), 170-175.
Leave a Reply