As the novel coronavirus continues to spread across the world, global health organizations have begun to identify patterns of uniquely susceptible populations.
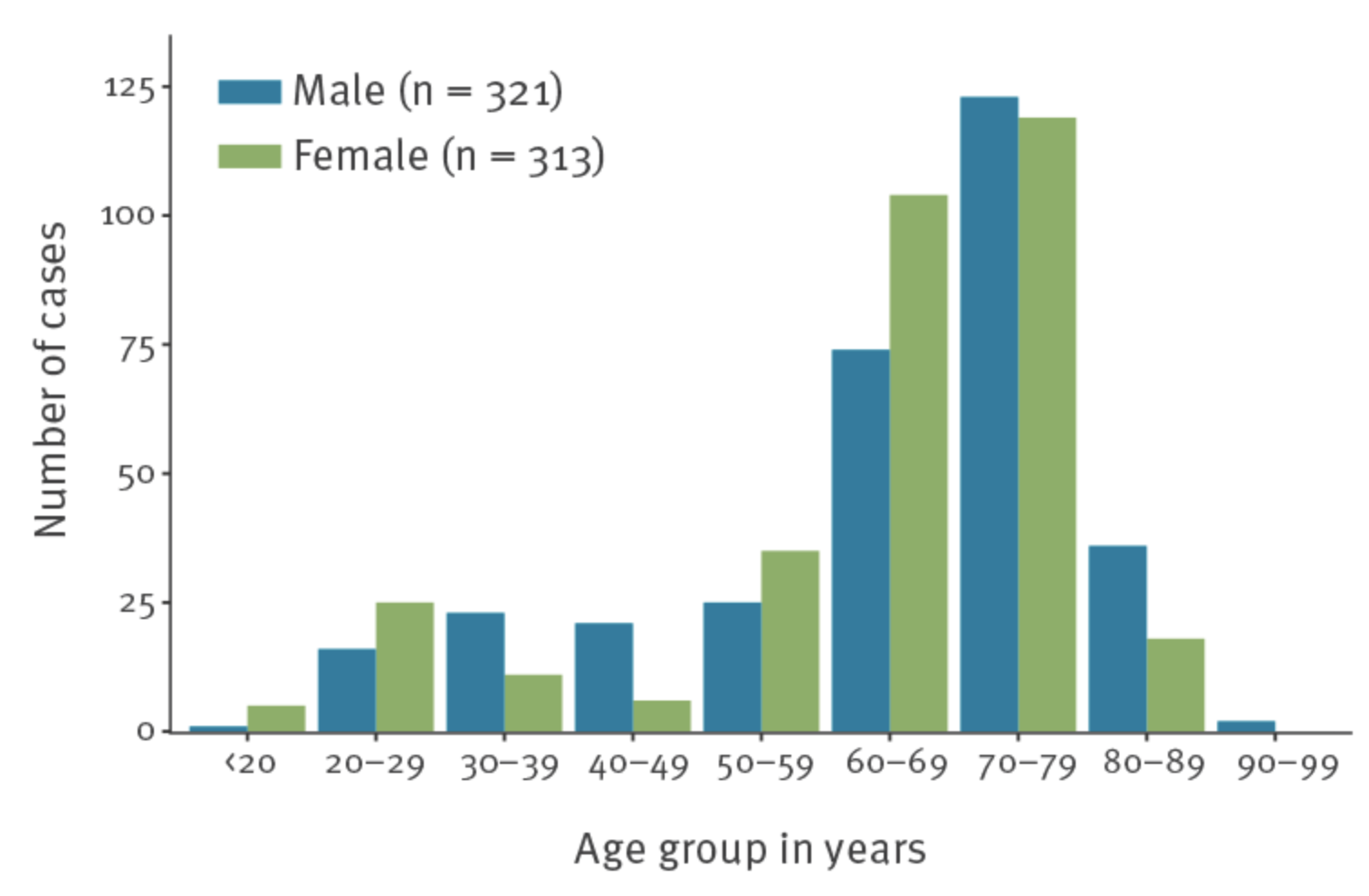
When discussing the epidemiology of this virus, it is important to distinguish between SARS-CoV-2 infection and the development of the COVID-19 disease. Approximately 50% of people who become infected with the virus do not develop any disease symptoms and may not know they have been infected, although they are still contagious and able to infect others for a period of approximately two weeks following their exposure. The distinction between asymptomatic and symptomatic patients is particularly important because, in situations where entire populations are tested en masse, there appears to be no sex difference in infection rates (4,5). For example, when the cruise ship Diamond Princess was quarantined off of Yokohama, Japan in February of 2020, all 3,711 passengers were tested. In this population, 634 tested positive for SARS-CoV-2 and of these, there was a roughly equal ratio between the sexes (50.6% male vs. 49.4% female) (Fig 1) (4). This finding has been confirmed by large-scale population testing in Iceland, where all citizens are subject to screening regardless of their symptomatic state (5).
While it appears that men and women are equally susceptible to becoming infected by the virus, it is evident that men are more likely to develop symptoms and become severely ill from their infection. The earliest studies of COVID-19 epidemiology in China indicated a male predisposition to developing severe complications from SARS-CoV-2 infection (1-3). This disposition has been maintained in later studies conducted across multiple countries, although the exact mechanism responsible remains unknown. As of April 1, 2020, statistics kept by the Spanish National Epidemiological Surveillance Network showed that 64% of COVID-19 deaths were male (6). Furthermore, the Spanish data shows a notable sexual disparity in symptom severity, wherein women who contract the virus are less likely to require hospitalization and men are more likely to require intensive care (Fig. 2).

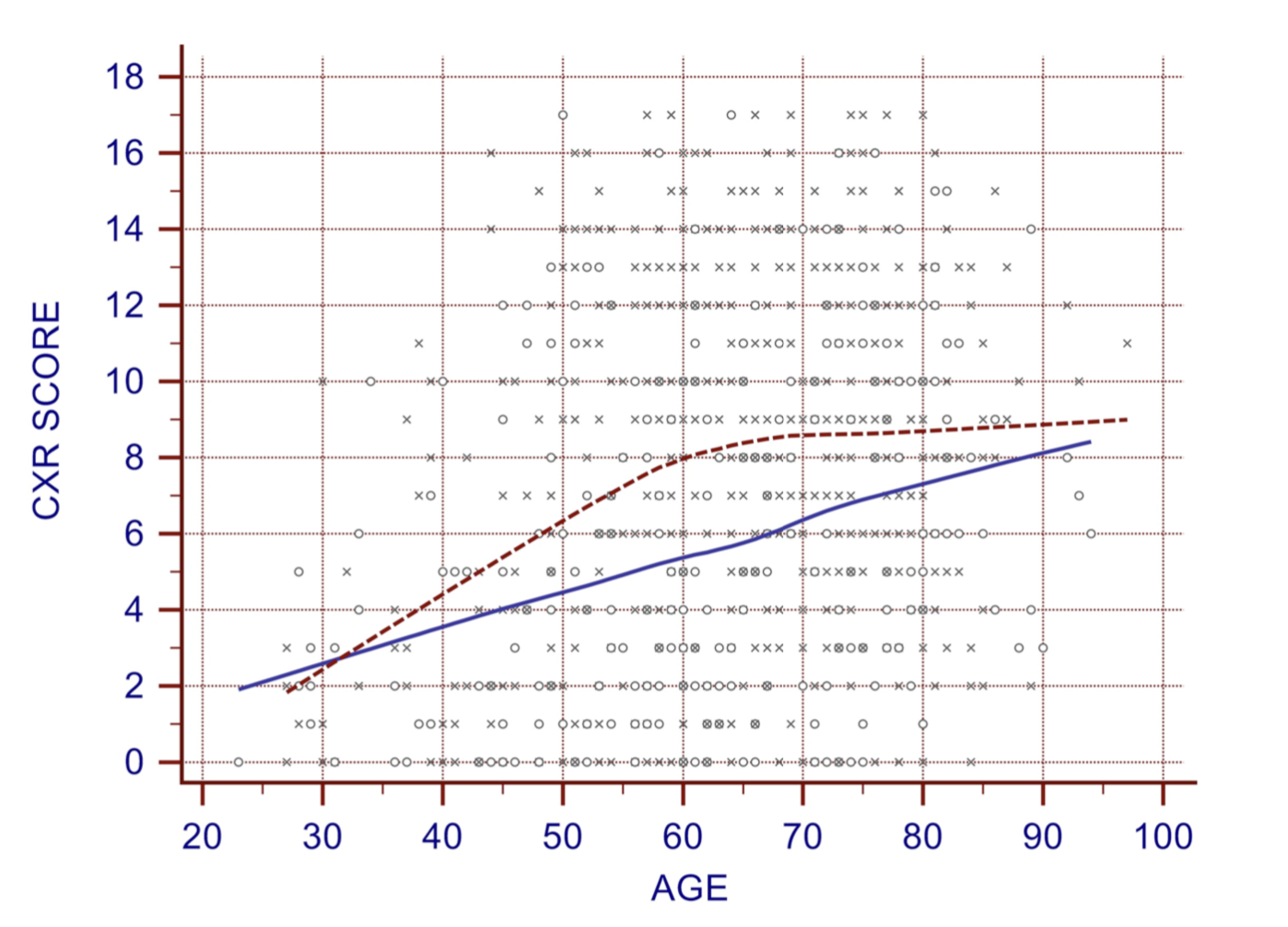
These epidemiological patterns have been repeated across the world in infected regions. In Italy, the virus has a 13.3% mortality rate among men compared to a 7.4% rate among women. Overall, 69.1% of fatalities in Italy have been male (7). Clinical studies have identified more severe disease indicators among male patients regardless of survival rate, including an Italian study of chest X-rays from COVID-19 patients demonstrating more severe lung damage among male patients compared to age-matched female patients (Fig. 3). Such studies combined with epidemiological patterns indicate an interaction between age and sex in susceptibility to severe illness from SARS-CoV-2 infection. While older individuals are at higher risk for developing respiratory problems requiring hospitalization and intensive care, this risk is exacerbated in males, who experience a higher risk at an earlier age compared to females.
Finally, it is important to note that the bias toward more severe disease in males seems to be consistent across age groups, as pediatric COVID-19 studies from both China (9) and the United States (10) have found that approximately 57% of SARS-CoV-2 positive symptomatic children are male. This strongly indicates that there is a genetic component to the male predisposition toward severe illness. Socio-behavioral factors such as diet or smoking rates have been proposed for the sex difference in COVID-19 severity, but these are insufficient to explain the discrepancy seen across cultures and age groups. Further study and expanded testing of asymptomatic populations will be necessary to fully elucidate the risk profile of SARS-CoV-2 infection and the development of COVID-19 disease symptoms.
Written by: Blaine Caslin
Edited by: Jina Zhou and Esther Melamed
4/13/2020
References
- Zhang JJ, Dong X, Cao Y, et al. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020; published online Feb 19.
- Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020; published online Feb 24.
- Guan W, Ni Z, Liang W, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020; published online Feb 28.
- Mizumoto Kenji , Kagaya Katsushi , Zarebski Alexander , Chowell Gerardo . Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19)cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Euro Surveill. 2020;25(10):pii=2000180.
- Berghildur skrifar – Um Helmingur Greindra Í Skimun Einkennalaus Eða Einkennalítill -Vísirhttps ://www.visir.is/g/2020140116d/um-helmingur-greindra-i-skimun-einkennalaus-eda-einkennalitill
- Informe nº 19. Situación de COVID-19 en España a 1 de abril de 2020. Equipo COVID-19. RENAVE. CNE. CNM (ISCIII)
- “Epidemia COVID-19” (PDF). epicentro.iss.it (in Italian). Istituto Superiore di Sanità. 30 March 2020. Retrieved 2 April 2020.
- Borghesi et al. Radiographic severity index in COVID-19 pneumonia: relationship to age and sex in 783 Italian patients. Nuclear Medicine & Medical Imaging 2020. Published online 27 March 2020.
- Dong Y, Mo X, Hu Y, et al. Epidemiology of COVID-19 Among Children in China. Pediatrics. 2020;145(6):e20200702
- Coronavirus Disease 2019 in Children — United States, February 12–April 2, 2020. MMWR Morb Mortal Wkly Rep. ePub: 6 April 2020. DOI: http://dx.doi.org/10.15585/mmwr.mm6914e4
Leave a Reply