The current evidence for a male predisposition toward increased risk of severe disease from SARS-CoV-2 infection is consistent across age groups and cultural demographics. Smoking was examined as a possible risk factor based on early studies on COVID-19 epidemiology out of China, where the noticable sex difference in disease severity was paired with a national difference in smoking rates between males and females. Approximately 50% of Chinese men smoke compared to ~2% of women according to the WHO, and this was posited as a potential explanation for the male predisposition to COVID-19 (1). However, data from Italy and Spain have indicated that this sexual disparity persists in countries with less egregious differences in smoking rates between sexes (2,3). Additionally, examination of pediatric COVID-19 cases from the United States and China have found that males are disproportionately represented among children who present COVID-19 symptoms (4,5), suggesting that the origin of this disparity is biological rather than behavioral.
Although it is still too early to tell exactly what is causing this sex difference in susecptibility to SARS-Cov-2, the related virus SARS-CoV-1 has been under investigation for a longer period of time and may shed some light on the potential mechanisms of the current pandemic. The 2002-2004 SARS outbreak in Southeast Asia showed similar sex patterns to the current COVID-19 pandemic, and researchers have been able to develop animal models to examine the infection profile. In a 2017 study, researchers found that male mice infected with a modified version of SARS-CoV-1 had a higher mortality rate than their female counterparts (6).
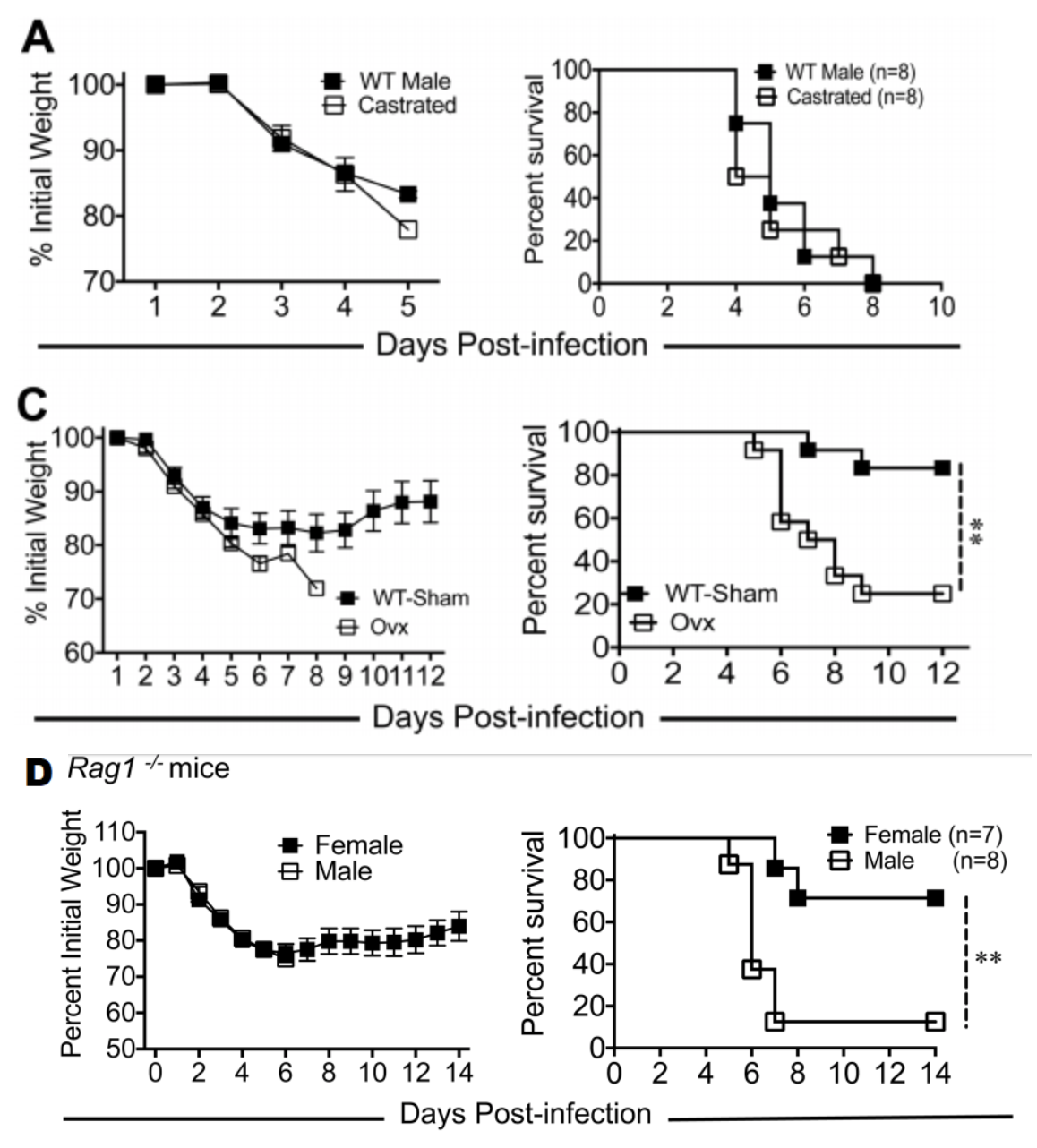
This pattern was seen in transgenic mice with a Rag1 knockout mutation, which do not produce mature T or B cells, indicating that the sexual disparity exists independently of underlying sex differences in the adapative immune system. However, gonadectomy of female wild-type mice removed this protective survival effect while gonadectomy of male mice did not affect survival rates. This suggests that the relative protection afforded to female SARS-CoV-1 patients is mediated through estrogen receptor signalling, although further research will be needed to validate these findings in SARS-CoV-2 infections and to fully elucidate the responsible mechanism (6).
Written by: Blaine Caslin
Edited by: Jina Zhou and Esther Melamed
4/20/2020
References
- Sex difference and smoking predisposition in patients with COVID-19. Lancet 2020. Published Online March 11, 2020 https://doi.org/10.1016/ S2213-2600(20)30117-X
- Informe nº 19. Situación de COVID-19 en España a 1 de abril de 2020. Equipo COVID-19. RENAVE. CNE. CNM (ISCIII)
- “Epidemia COVID-19” (PDF). epicentro.iss.it (in Italian). Istituto Superiore di Sanità. 30 March 2020. Retrieved 2 April 2020.
- Liu, et al. Detection of Covid-19 in Children in Early January 2020 in Wuhan, China. New England Journal of Medicine 2020.
- Coronavirus Disease 2019 in Children — United States, February 12–April 2, 2020. MMWR Morb Mortal Wkly Rep 2020;69:422–426. DOI: http://dx.doi.org/10.15585/mmwr.mm6914e4
- Channappanavar et al. Sex-Based Differences in Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Infection. J Immunol May 15, 2017, 198 (10) 4046-4053; DOI: https://doi.org/10.4049/jimmunol.1601896
Leave a Reply