Written by: Parker Davis
Edited by: Esther Melamed
Anosmia and ageusia – a loss of the sense of smell and taste, respectively – are well-documented symptoms of infection by SARS-CoV-2, the agent of COVID-19 (Vaira et al., 2020; Mak et al., 2020; Tanasa et al., 2020). Though the origins of these symptoms were initially somewhat mysterious, several hypotheses for their pathogenesis have been put forth: it is known, for example, that angiotensin-converting enzyme 2 – the putative receptor for SARS-CoV-2 – is found in large quantities in mucosal linings of the mouth and tongue, as well as in the nasal mucosa (Vaira, Salzano, Fois, Piombino, 2020). The authors hypothesize that disruptions in signaling pathways and the death of cells in these mucosae may be responsible for the loss of the senses. Additionally, Kanjanaumporn et al. have posited that anosmia may be due to the infection and destruction of glial cells in the brain that support olfaction, rather than of olfactory sensory neurons directly (Kanjanaumporn et al., 2020). In addition, many COVID-19 patients have presented with neurological symptoms including headaches and altered mental status; MRI findings in patients with these symptoms exhibit abnormal activation of many areas of the brain (Solomon et al., 2020; Kandemirli et al., 2020). These findings set the stage for investigation of the neurological effects of COVID-19.
In a paper published this past January in JAMA Neurology, Ismail and Gad used functional magnetic resonance imaging (fMRI) to observe activation of brain areas in a single patient who developed cacosmia and cacogeusia (a persistent bad smell or taste, respectively, not associated with any specific food, drug, or other substance) following SARS-CoV-2 infection. Physical and CT examinations did not yield any abnormal findings in the ears, nose, throat, or paranasal sinuses. Additionally, findings from a follow-up neurological exam were normal. Initial MRI revealed normal structural and signal findings of the olfactory bulbs and sulci. The authors then subjected the patient to a task-based fMRI, in which activation of different regions of the brain could be monitored and measured based on the amount of blood flow through a given region during the task. Using T1- and T2-weighted images, they noted a lack of blood oxygen level-dependent (BOLD) activation in the orbitofrontal cortex (OFC), a secondary region of olfaction and tertiary region of gustation (Figure 1B); and they noted strong BOLD activation in the right uncus/piriform cortex, primary brain regions of olfaction (Figure 2).
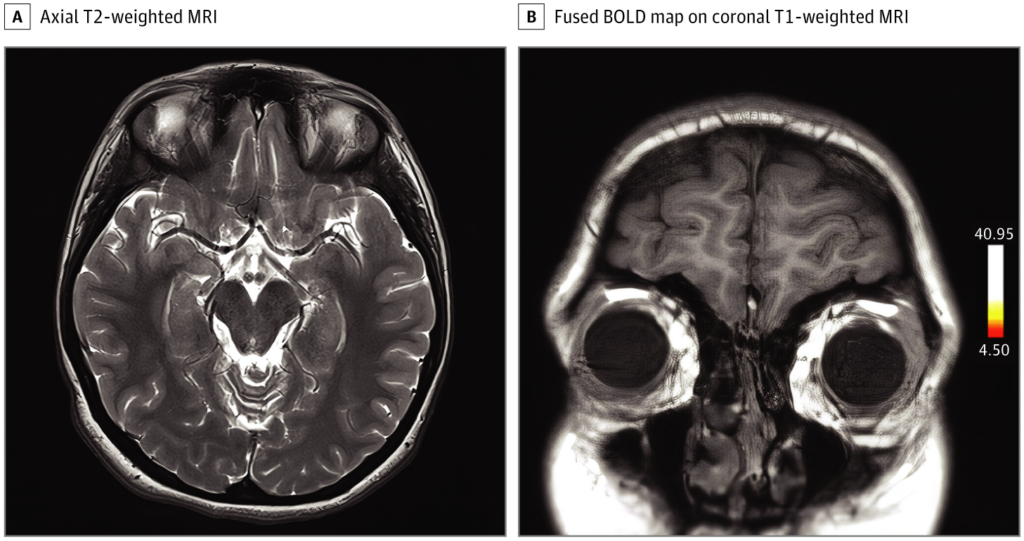
Figure 1. A) Axial T2-weighted image at the level of medial temporal lobes, gyrus rectus, and orbitofrontal gyrus showing no structural or signal abnormalities. B) Fused BOLD map on coronal T1-weighted image showing no activation in the region of the OFC. (Ismail, Gad, 2021)

[Figure 2. A) Fused BOLD map on coronal T1-weighted image showing activation of the right uncus at the region of piriform cortex and at the anterior cingulate. B) Fused BOLD map on axial T1-weighted image showing two sites of activation of the right uncus at the region of piriform cortex. (Ismail, Gad, 2021)]
Though olfactory dysfunction is common in respiratory virus infections, in such infections it is typically secondary to other causes, such as nasal congestion or a runny nose. However, COVID-19 is not usually associated with these primary symptoms. Thus, the underlying cause of anosmia, cacosmia, and other parosmias in COVID-19 is thought to be the brain-seeking behavior of the virus itself (Ton et al., 2020). The findings outlined here are in line with previous evidence of patterns of brain activation as a result of SARS-CoV-2 infection: many studies have implicated the OFC with olfactory dysfunction in these patients, with some showing hypoactivity and others showing extreme hyperintensity of subregions on fMRI and electroencephalography (EEG) (Guennec et al., 2020; Politi, Salsano, Grimaldi, 2020). Despite discrepancies in the exact findings, these studies show clearly that the virus influences olfaction – and likely gustation – via modulation of brain activity at the sites of sensation and perception. Whether the virus itself actually invades the brain, or simply acts from a distance, has not yet been determined. If it does invade, it is likely through the olfactory pathway, leaving in its wake a malodorous trail of destruction.
References
Ismail, I. I., & Gad, K. A. (2021). Absent Blood Oxygen Level-Dependent Functional Magnetic Resonance Imaging Activation of the Orbitofrontal Cortex in a Patient with Persistent Cacosmia and Cacogeusia after COVID-19 Infection. JAMA Neurology. American Medical Association.
Kandemirli, S. G., Dogan, L., Sarikaya, Z. T., Kara, S., Akinci, C., Kaya, D., Kaya, Y., Yildirim, D., Tuzuner, F., Yildirim, M. S., Ozluk, E., Gucyetmez, B., Karaarslan, E., Koyluoglu, I., Demirel Kaya, H. S., Mammadov, O., Ozdemir, I. K., Afsar, N., Yalcinkaya, B. C., … Kocer, N. (2020). Brain MRI findings in patients in the intensive care unit with COVID-19 infection. Radiology, 297(1), E232–E235.
Kanjanaumporn, J., Aeumjaturapat, S., Snidvongs, K., Seresirikachorn, K., & Chusakul, S. (2020). Smell and taste dysfunction in patients with SARS-CoV-2 infection: A review of epidemiology, pathogenesis, prognosis, and treatment options. Asian Pacific Journal of Allergy and Immunology (Vol. 38, Issue 2, pp. 69–77).
Le Guennec, L., Devianne, J., Jalin, L., Cao, A., Galanaud, D., Navarro, V., Boutolleau, D., Rohaut, B., Weiss, N., & Demeret, S. (2020). Orbitofrontal involvement in a neuroCOVID-19 patient. Epilepsia, 61(8), e90–e94.
Mak, P. Q., Chung, K. S., Wong, J. S. C., Shek, C. C., & Kwan, M. Y. W. (2020). Anosmia and ageusia: Not an uncommon presentation of COVID-19 infection in children and adolescents. Pediatric Infectious Disease Journal, 39(8), E199–E200.
Politi, L. S., Salsano, E., & Grimaldi, M. (2020). Magnetic resonance imaging alteration of the brain in a patient with coronavirus disease 2019 (COVID-19) and anosmia. JAMA Neurology (Vol. 77, Issue 8, pp. 1028–1029). American Medical Association.
Solomon, I. H., Normandin, E., Bhattacharyya, S., Mukerji, S. S., Keller, K., Ali, A. S., Adams, G., Hornick, J. L., Padera, R. F., & Sabeti, P. (2020). Neuropathological Features of Covid-19. New England Journal of Medicine, 383(10), 989–992.
Tanasa, I., Manciuc, C., Carauleanu, A., Navolan, D., Bohiltea, R., & Nemescu, D. (2020). Anosmia and ageusia associated with coronavirus infection (COVID‑19) – what is known? Experimental and Therapeutic Medicine, 20(3), 2344–2347.
Tong, J. Y., Wong, A., Zhu, D., Fastenberg, J. H., & Tham, T. (2020). The Prevalence of Olfactory and Gustatory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis. Otolaryngology – Head and Neck Surgery (United States) (Vol. 163, Issue 1, pp. 3–11). SAGE Publications Inc.
Vaira, L. A., Salzano, G., Deiana, G., & De Riu, G. (2020). Anosmia and Ageusia: Common Findings in COVID-19 Patients. Laryngoscope, 130(7), 1787.
Vaira, L. A., Salzano, G., Fois, A. G., Piombino, P., & De Riu, G. (2020). Potential pathogenesis of ageusia and anosmia in COVID-19 patients. International Forum of Allergy and Rhinology (Vol. 10, Issue 9, pp. 1103–1104). John Wiley and Sons Inc.
Leave a Reply